Obesity
ΕΤΥΜΟΛΟΓΙΑ
Latin:Obesus - fatExcess weight. Arbitrarily defined as a BMI >30. Generally a result of excess calorie intake in relation to energy expenditure. In England, the Health Survery showed that 23.8% of the population was classified as obese.
Distribution of body mass may also be important, with some evidence suggesting that a "pear-shaped" fat distribution - with the fat predominantly on the buttocks and legs - may be less associated with some diseases than an "apple-shaped" fat distribution, with more abdominal fat; or that waist measurements may be more significant than body weight. Whatever wrist to hip ratio (WHR) is a better predictor of mortality than BMI over 14 years follow-up[1]
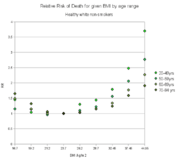
Apart from mortality which as a "J shaped" relationship to BMI[2], obesity increases the risk of several other conditions with most of the cardiovascular risk being related in turn to secondary diabetes mellitus and hypertension.
- Hypertension
- Diabetes mellitus
- Osteoarthritis
- Cardiovascular disease (BMI is NOT an independent risk factor for mortality)
- Obstructive sleep apnoea
- Dyspepsia (and see below for risk of continued reflux)
-
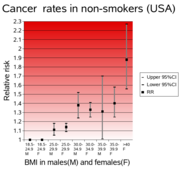
Cancer - BMI is independent risk factor for mortality
- Most of excess risk with BMI > 40
-
Cancers whose risk most increased are:[3]
- Uterine cancer in women
- Liver cancer in men
- Kidney cancer in woman
- Cervical cancer in woman
- Pancreatic cancer both sexes
- Oesophageal cancer both sexes
Contents |
Aetiology
Extremely complex interaction between genetics, environment and individual behaviour. Examples of such factors follow to give a flavour rather than suggest any are important in an individual. The hypothalamic leptin/melanocortin pathway is only thought to be important in a minority. There is a strong genetic component (40 to 80% heritability).
Genetics
The strongest genomewide associations of body mass index are with introns 1 and 2 of the gene FTO. This modulates a pathway of adipocyte thermogenesis regulation coded by genes including ARID5B, IRX3, and IRX5[4]. Mitochondrial thermogenesis is also regulated by the genes that control the expression of uncoupling protein 1 coded by UCP1 which include IRF4, PRDM16, and TBX15.
Monogenetic
- Melanocortin 4 receptor (MC4R) mutations[5] - commonest monogenetic cause of obesity -adult prevalence in the extremely obese about 2.5%[6]
- Leptin deficiency[7][8]
- Leptin receptor (LEPR) deficiency[9]
- Pro-opiomelanocortine (POMC) gene
- Prohormone convertase 1 (PC1) gene
Polygenetic
- Prader-Willi syndrome
- Bardet-Biedl syndrome
- Β-3 adrenergic receptor varients in women
- Uncoupling protein-1
- Regulator regions of the leptin gene
- Low-density lipoprotein receptor in women
- Tumour necrosis factor alpha in women
- INSIG2 gene[10]
Environment
- Gut microflora[11]
- Dietary habits[12],
- Sedentarism
- Β 2-adrenoceptors and physical activity in woman
- Antipsychotics[13]
Behaviour
Social class/status is almost as greater a predictor of obesity as any other factor. The fact that eating behaviour can be genetically determined in some[14]is not believed to be a major cause of this association. The only social group in Britain as of not getting more obese is professional women, emphasizing perhaps a consistency in behaviour of this social grouping over the last few decades[15].
- Intake of high energy foods
- Intake alcohol
Treatment
You might as well keep it simple because they all work if you stick with them ![16]
- Diet and exercise[17][18]
-
Drugs. There are no magic pills. Indeed more drugs have been withdrawn from market in this indication recently than most others.
- Appetite suppressant
- Drugs that reduce intestinal absorption
-
Bariatric surgery[19]
- Works but takes at least three years to give return on investment from health economic point of view
Obesity as a contraindication to treatment
Obesity may:
- Reduce the likelihood that a treatment will work, sometimes to the extent that it is not worth providing, or may not be cost-effective.
- Increase the risk of adverse reactions.
Obesity may therefore be a relative or absolute contraindication. However for interventions such as total hip replacement, once all the other conditions associated with obesity such as ischaemic heart disease and diabetes are corrected for, being over weight is probably protective[20].
For example, when considering the use of combined oral contraceptives:[21]
- A body mass index of Body mass index ≥ 30 - 34 kg/m2 comprises "A condition where the advantages of using the method generally outweigh the the theoretical or proven risks";
- A body mass index 35 – 39 kg/m2 comprises "A condition where the theoretical or proven risks usually outweigh the advantages of using the method"; and
- A body mass index ≥ 40 kg/m2 comprises "A condition which represents an unacceptable health risk if the contraceptive method is used".
Treatments that do not work
Weight loss is associated with smoking. However the risks of the treatment (smoking) easily outweighs the benefit in terms of weight reduction. Mortality in diabetic smokers and non-smokers has been explored in detail as a function of body mass index. Once early deaths are eliminated we find that the J shaped curve in mortality as related to BMI is almost totally driven by low BMI smokers. Non smokers have a close to linear relationship between BMI and increased mortality[22]. In other words those diabetics with a low body mass index (BMI between 18.5 to 22.4) and who smoke are at much higher risk of mortality than those diabetics whose BMI is low for non pathological reasons.
References
- ↑ Sahakyan KR, Somers VK, Rodriguez-Escudero JP, Hodge DO, Carter RE, Sochor O, Coutinho T, Jensen MD, Roger VL, Singh P, Lopez-Jimenez F. Normal-Weight Central Obesity: Implications for Total and Cardiovascular Mortality. Annals of internal medicine. Dec 1; 163(11):827-35.(Link to article – subscription may be required.)
- ↑ Adams KF, Schatzkin A, Harris TB, Kipnis V, Mouw T, Ballard-Barbash R, Hollenbeck A, Leitzmann MF. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med.355(8):763-78.
- ↑ Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. The New England journal of medicine;348:1625-38.(Direct link – subscription may be required.)
- ↑ Claussnitzer M, Dankel SN, Kim KH, Quon G, Meuleman W, Haugen C, Glunk V, Sousa IS, Beaudry JL, Puviindran V, Abdennur NA, Liu J, Svensson PA, Hsu YH, Drucker DJ, Mellgren G, Hui CC, Hauner H, Kellis M. FTO Obesity Variant Circuitry and Adipocyte Browning in Humans. The New England journal of medicine. Sep 3; 373(10):895-907.(Link to article – subscription may be required.)
- ↑ Farooqi IS, Keogh JM, Yeo GS, Lank EJ, Cheetham T, O'Rahilly S. Clinical spectrum of obesity and mutations in the melanocortin 4 receptor gene. The New England journal of medicine;348:1085-95. (Direct link – subscription may be required.)
- ↑ Lubrano-Berthelier C, Dubern B, Lacorte JM, Picard F, Shapiro A, Zhang S, et al. Melanocortin 4 receptor mutations in a large cohort of severely obese adults: prevalence, functional classification, genotype-phenotype relationship, and lack of association with binge eating. The Journal of clinical endocrinology and metabolism;91:1811-8. (Direct link – subscription may be required.)
- ↑ Gibson WT, Farooqi IS, Moreau M, DePaoli AM, Lawrence E, O'Rahilly S, Trussell RA. Congenital leptin deficiency due to homozygosity for the Delta133G mutation: report of another case and evaluation of response to four years of leptin therapy. The Journal of clinical endocrinology and metabolism. Oct; 89(10):4821-6.(Link to article – subscription may be required.)
- ↑ Farooqi IS, Keogh JM, Kamath S, Jones S, Gibson WT, Trussell R, Jebb SA, Lip GY, O'Rahilly S. Partial leptin deficiency and human adiposity. Nature. Nov 1; 414(6859):34-5.(Link to article – subscription may be required.)
- ↑ Farooqi IS, Wangensteen T, Collins S, Kimber W, Matarese G, Keogh JM, et al. Clinical and molecular genetic spectrum of congenital deficiency of the leptin receptor. The New England journal of medicine;356:237-47. (Direct link – subscription may be required.)
- ↑ Herbert A, Gerry NP, McQueen MB, Heid IM, Pfeufer A, Illig T, et al. A common genetic variant is associated with adult and childhood obesity. Science;312:279-83. (Direct link – subscription may be required.)
- ↑ Turnbaugh PJ, Ley RE, Mahowald MA, Magrini V, Mardis ER, Gordon JI. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature;444:1027-31. (Direct link – subscription may be required.)
- ↑ Santos JL, Boutin P, Verdich C, Holst C, Larsen LH, Toubro S, et al. Genotype-by-nutrient interactions assessed in European obese women : A case-only study. European journal of nutrition;45:454-62. (Direct link – subscription may be required.)
- ↑ Chagnon YC. Susceptibility genes for the side effect of antipsychotics on body weight and obesity. Curr Drug Targets.7(12):1681-95
- ↑ Branson R, Potoczna N, Kral JG, Lentes KU, Hoehe MR, Horber FF. Binge eating as a major phenotype of melanocortin 4 receptor gene mutations. The New England journal of medicine;348:1096-103. (Direct link – subscription may be required.)
- ↑ Fair Society, Healthy Lives - The Marmot Review Final Report
- ↑ Thomas SL, Hyde J, Karunaratne A, Kausman R, Komesaroff PA. "They all work...when you stick to them": a qualitative investigation of dieting, weight loss, and physical exercise, in obese individuals. Nutrition journal. 7:34.(Epub) (Link to article – subscription may be required.)
- ↑ Poirier P, Després JP. Exercise in weight management of obesity. Cardiology clinics. Aug; 19(3):459-70.
- ↑ Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, Stearns SC, Smith WC, Jung RT, Campbell MK, Grant AM. Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement. Health technology assessment (Winchester, England). May; 8(21):iii-iv, 1-182.
- ↑ Picot J, Jones J, Colquitt JL, Gospodarevskaya E, Loveman E, Baxter L, Clegg AJ. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Health technology assessment (Winchester, England). Sep; 13(41):1-190, 215-357, iii-iv.(Link to article – subscription may be required.)
- ↑ Hunt LP, Ben-Shlomo Y, Clark EM, Dieppe P, Judge A, MacGregor AJ, Tobias JH, Vernon K, Blom AW. 90-day mortality after 409,096 total hip replacements for osteoarthritis, from the National Joint Registry for England and Wales: a retrospective analysis. Lancet. Sep 28; 382(9898):1097-104.(Link to article – subscription may be required.)
- ↑ Clinical Effectiveness Unit of the Faculty of Family Planning and Reproductive Heath Care. UK medical eligibility for contraceptive use (UKMEC). London: Faculty of Family Planning and Reproductive Heath Care of the Royal College of Obstetricians and Gynaecologists, (see p13)
- ↑ Tobias DK, Pan A, Jackson CL, O'Reilly EJ, Ding EL, Willett WC, Manson JE, Hu FB. Body-mass index and mortality among adults with incident type 2 diabetes. N Engl J Med. Jan 16;370(3):233-44. doi: 10.1056/NEJMoa1304501.